
Obsessive Compulsive Disorder (OCD)
Obsessive-Compulsive Disorder is a mental health condition involving persistent, intrusive, and distressing thoughts or images that are not in line with what a person wants (obsessions) that are followed by behaviors or thinking patterns (compulsions) that are intended to reduce distress.
People with OCD typically feel like they have to engage in their compulsions, such as washing their hands repeatedly, reassurance seeking, rituals, rumination, or checking behaviours to alleviate the anxiety or fear caused by their obsessions. Compulsions tend to become more and more time-consuming over time and interfere with daily life, relationships, and work.
People with OCD typically feel like they have to engage in their compulsions, such as washing their hands repeatedly, reassurance seeking, rituals, rumination, or checking behaviours to alleviate the anxiety or fear caused by their obsessions. Compulsions tend to become more and more time-consuming over time and interfere with daily life, relationships, and work.
Themes of OCD
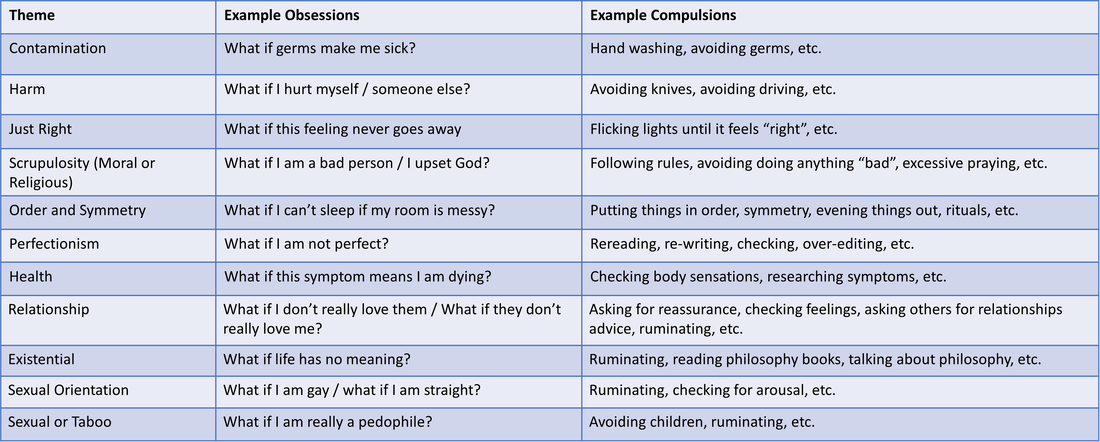
Obsessions can vary widely from person to person. Over time the the themes of obsessions that a person experiences can shift if OCD is left untreated. Some common OCD themes are listed in the table below:
OCD Cycle
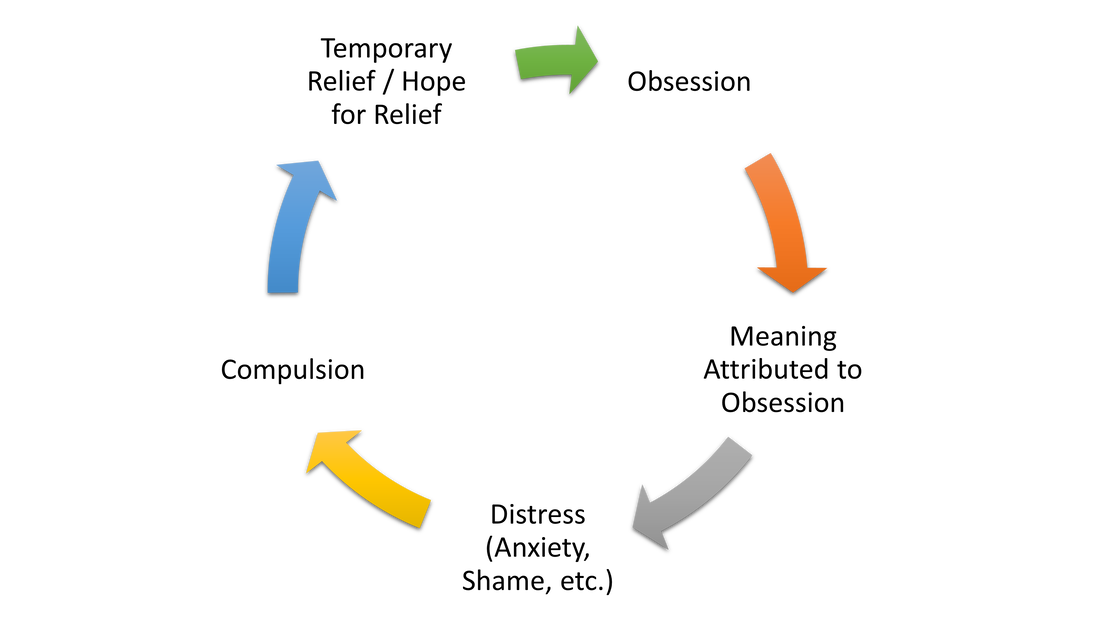
If left untreated, OCD symptoms tend to worsen over time. This is because OCD involves a cycle in which individuals feel compelled to engage in repetitive behaviors or mental acts (compulsions) in response to unwanted, intrusive thoughts or images (obsessions). Although these compulsions may provide temporary relief or hope for relief, they can significantly impact people's ability to engage in activities that they value in their lives. Furthermore, the relief provided by the compulsions is only temporary, and the obsessions and distress tend to return, leading to a repeating cycle. The diagram below provides a visual representation of the OCD cycle.
Exposure and Response Prevention
Our approach to treating OCD is guided by psychological research. Thus, our primary method of treatment is Exposure with Response Prevention (ERP), a form of Cognitive Behavioral Therapy that is considered the gold standard for treating OCD. ERP is designed to help clients systematically and gradually break the cycle of OCD by facing their fears and learning new ways to respond to triggers. By resisting the urge to engage in compulsive behaviors or mental acts, clients can gain more flexibility in their lives and reduce the impact of OCD on their daily activities. We work collaboratively with our clients to create a supportive and safe environment for the ERP process, ensuring that clients feel comfortable and motivated throughout treatment.
Acceptance and Commitment Therapy (ACT) is a form of cognitive-behavioral therapy that can be used to treat OCD. ACT focuses on increasing psychological flexibility by promoting acceptance of unwanted experiences and taking committed action towards meaningful goals. ACT can be integrated into OCD treatment in a number of ways. For example, ACT emphasizes the importance of identifying and committing to personal values as a way to guide behavior. By clarifying their values, individuals with OCD can commit to engaging in behaviours that are in line with their values, even in the presence of anxiety or distress. We can also integrate individuals' values in their ERP work, making this work more personally meaningful. Another way, that ACT can be integrated into OCD treatment is with diffusion. Diffusion involves learning to distance oneself from one's thoughts and view them as mental events rather than objective reality. In the context of OCD, diffusion can help individuals see their obsessions as mere thoughts, rather than absolute truths that require compulsive behaviors to alleviate anxiety.
Other Approaches for Treating OCD: Inference Based CBT (IB-CBT)
Inference-Based Cognitive Behavioral Therapy (IB-CBT) is an newer approach to treating OCD that focuses on identifying and addressing the underlying cognitive processes that contribute to obsessive-compulsive symptoms. Unlike traditional CBT approaches, IB-CBT emphasizes the role of inference, or the process of drawing conclusions based on incomplete information, in maintaining OCD symptoms. This approach targets inferential processes and helps individuals become more aware of their own thinking patterns (meta-cognition), which is believed to help individuals be able to unhook from these thoughts. Research on IB-CBT for OCD is still relatively limited, but the available studies have shown promising results. This approach can be helpful to clients who have not responded well to ERP.
OCD Therapy
We view therapy as a collaboration, and therefore we take an active role when working with our clients. In sessions, we help you apply strategies and skills and provide you with the opportunity to practice these skills between sessions. Although we focus on providing you with latest treatment approaches, we also aim to help you feel confident in this work and we find ways to make the process fun, especially when working with children and teens.
OCD Resources
- The International OCD Foundation has a wealth of resources, research, and videos to help you learn more about obsessive compulsive disorder.
- Unstuck: is a documentary about six kids living with OCD. It can provide a great deal of hope for children.
- AnxietyCanada provides information on OCD.
- Kids IOCDF is a website that focuses specifically on the topic of pediatric OCD.
- IOCDF has a very comprehensive reading list for OCD and an excellent list of OCD books (and workbooks for kids).


